

Abstract
Background: Isocitrate dehydrogenase 1 mutations (IDH1m) occur in 7-14% of AML patients and 3% of MDS patients and produce 2-hydroxyglutarate (2-HG), an oncometabolite that impairs differentiation. FT-2102 is an oral, highly potent, selective small molecule inhibitor of mutated IDH1, with the therapeutic potential to restore normal cellular differentiation. Herein, we present preclinical and clinical data from an ongoing Phase 1/2 study of single-agent (SA) FT-2102 in patients with IDH1m AML and MDS (CT.gov: NCT02719574).
Methods: Extensive pre-clinical evaluations were performed on FT-2102, including CYP interactions in-vivo in rat and in-vitro in human tissue and in-vivo QTc toxicology in monkeys. The clinical Phase 1 study was initiated to evaluate the safety, PK/PD, and antileukemic activity of FT-2102 in patients with IDH1m AML or MDS and included both dose escalation and expansion phases. FT-2102 was administered daily until disease progression or unacceptable toxicity. Eligibility criteria included: IDH1m AML/MDS [relapsed/refractory (R/R) or treatment naïve (TN) for whom standard therapy was contraindicated], adequate liver and renal function, no prior IDH1 inhibitors, and no restrictions for concomitant non-anticancer medications. Investigator-assessed responses were per modified IWG 2003/2006 criteria. Efficacy was assessed at Cycle 2 Day 1 and as clinically indicated thereafter. Adverse events (AEs) were assessed throughout the study per NCI CTCAE version 4.03.
Results: Evaluation of FT-2102 in in-vivo rat and in-vitro human tissue indicated hepatic metabolism by CYP enzymes (CPY3A4, 2C9, 1A1) as the major route of excretion. Animal toxicology studies predicted the threshold for QTc risk occurred at exposures >5.5 fold higher than the murine exposure at which 90% 2-HG reduction was observed.
In the clinical study, at the time of the data cutoff, 31 patients (pts) had been treated with SA FT-2102, with a median of 3 mo. on treatment (range: 0.2 to 20 mo.). Of the 31pts treated, 25 had AML (22 R/R; 3 TN) and 6 had MDS (4 R/R; 2 TN). The median number of prior anti-leukemia therapies was 2 (range: 0-9) for AML pts and 1 (range: 0-4) for MDS pts. FT-2102 doses were: 150 mg QD (n=8), 300 mg QD (n=4), 150 mg BID (n=16), and 100 mg QD with food (n=3). Eighteen pts discontinued treatment, most commonly due to death (n=5), progressive disease (n=5), HSCT (n=3), or lack of response (n=3).
Severe (≥Grade 3) AEs occurring in >5% of pts included thrombocytopenia (26%), febrile neutropenia (23%), anemia (19%), pneumonia (13%), neutropenia (7%), hypokalemia (7%), pyrexia (7%) and leukocytosis (6%). Three pts had differentiation syndrome (IDH-DS), which resolved with temporary interruption of FT-2102, treatment with dexamethasone, hydroxyurea, and supportive care in all three. One pt had transient QTcF prolongation (Grade 3) which resolved with temporary interruption of FT-2102 and cessation of suspected concomitant medications. Eight pts died on treatment or within 28 days of the last dose, with no deaths considered related to FT-2102. No DLTs were observed during dose escalation.
Selection of FT-2102 150 mg BID as the RP2D was supported by PK and PD data. Durable steady-state (Css) achieved by Week 2 was well below the threshold for QTc risk predicted by preclinical studies. The predicted IC90 was confirmed with prompt and durable 2-HG reduction to normal levels by C2D1 at the RP2D.
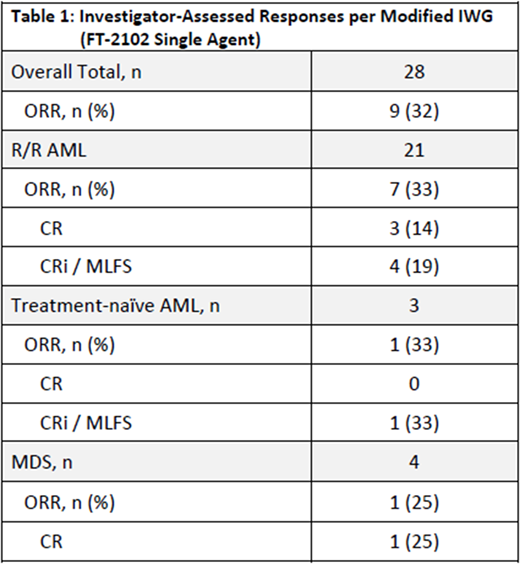
Table 1 shows the Investigator-assessed ORR per IWG. Responses have been observed from 1 to 6 months on treatment, with stable disease observed beyond 6 months; 42% of the patients remain on treatment.
Conclusions: FT-2102 preclinical evaluations suggest a low risk of clinically significant CYP-mediated drug-drug interaction and QTc prolongation. SA FT-2102 is well tolerated in AML and MDS, with 150 mg BID selected as the RP2D based on safety, PK and PD (2-HG) response. Significant clinical activity has been observed in heavily pre-treated and in TN patients, both in AML and MDS. FT-2102 continues being investigated at a dose of 150 mg BID in a Phase 2 study. Three SA Phase 2 cohorts are currently open for enrollment in R/R AML, AML/MDS with CR/CRi (i.e., with MRD), and in pts with R/R MDS/AML with prior exposure to an IDH1m inhibitor. Data updates will be available at the time of presentation.
Lee:LAM Therapeutics: Research Funding; Karyopharm Therapeutics Inc: Consultancy; AstraZeneca: Consultancy; Clinipace: Consultancy; Amgen: Consultancy. Schiller:Celator/Jazz Pharmaceuticals: Research Funding; Pharmacyclics: Research Funding. Ferrell:Incyte: Research Funding. Kelly:Forma Therapeutics Inc.: Employment. Li:Forma Therapeutics Inc.: Employment. Sweeney:Forma Therapeutics Inc.: Employment. Watson:Forma Therapeutics Inc.: Employment. Mohamed:Forma Therapeutics Inc.: Employment. Cortes:Pfizer: Consultancy, Research Funding; Daiichi Sankyo: Consultancy, Research Funding; Novartis: Consultancy, Research Funding; Astellas Pharma: Consultancy, Research Funding; Arog: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal